Epidemics can occur anywhere, at any time.
We publish regular updates, produced by Program for Monitoring Emerging Diseases (ProMED), on outbreaks of emerging infectious diseases to keep you informed on the frequency and impact of our priority diseases.
ProMED is the largest publicly-available system conducting global reporting of infectious diseases outbreaks, with ProMED staff, moderators and team members scanning for, reviewing and posting information relating to global health security from official health reports and media articles.
The below post contains information from health reports, news articles, and academic papers relating to our priority diseases, compiled together by ProMED. Content below may be edited from original ProMED posts for style and length.
These posts provide an overview of disease outbreak activity over the past several weeks. For the latest information relating to outbreaks of infectious diseases, please visit the ProMED website.
Ebola
Location
North Kivu and Ituri provinces, Democratic Republic of Congo
Outbreak Update
WHO Emergencies preparedness, response, Disease outbreak news, 2 August 2019:
The Ebola virus disease (EVD) outbreak in North Kivu and Ituri provinces in the Democratic Republic of the Congo continued this week with similar transmission intensity to recent weeks, with an average of 85 cases per week (range 79-91 cases per week) in the past 6 weeks. There are currently no confirmed cases of EVD outside of the Democratic Republic of the Congo.
On 30 Jul [2019], a confirmed EVD case was reported in Nyiragongo Health Zone on the outskirts of Goma city. The case worked as a miner in Ituri province and travelled down through several outbreak hotspots, where he likely acquired the disease. Currently, there is no indication that the case had links to the to the 1st case identified in Goma on 14 Jul [2019].
In the 21 days from 11-31 Jul 2019, 71 health areas within 18 health zones reported new cases, representing 11% of the 664 health areas within North Kivu and Ituri provinces (Table 1, Figure 2). During this period, a total of 260 confirmed cases were reported, with the majority coming from the health zones of Beni (52%, n=135) and Mandima (16%, n=41). Most (68%, n=28) of the cases reported in Mandima Health Zone came from Some Health Area, which has in turn seeded cases to the nearby city of Mambasa in recent weeks. The response in Some Health Area was challenging for several weeks due to tension between local communities and Ebola response teams. However, the situation has improved following dialogues with community leaders to understand the community's perspective and to define common ground for collaboration. Biena Health Zone recently cleared 21 days since their last reported case. However, hotspots continue to be the source of cases in other areas through the movement of suspected and confirmed cases and their contacts, and high risks remain for the virus to be reintroduced to these areas, requiring teams to remain fully resourced and vigilant.
As of 31 Jul 2019, a total of 2713 EVD cases were reported, including 2619 confirmed and 94 probable cases, of which 1823 cases died (overall case fatality ratio 67%). Of the total confirmed and probable cases, 56% (1527) were female, and 29% (773) were children aged less than 18 years. Cases continue to increase among health workers, with the cumulative number infected rising to 149 (5% of all confirmed and probable cases). 1 Aug 2019 marked one year since the government of the Democratic Republic of the Congo declared the Ebola outbreak.
See the full ProMED post here
Zika
Location
Brazil, Peru, China, USA
Outbreak Update
Brazil:
Sao Carlos, Sao Paulo state. 13 Jul 2019. 31 cases suspected
Minas Gerais state. 9 Jul 2019. 1006 probable cases.
Peru:
1 Aug 2019. 896 cases reported; health emergency declared in Jaen province, Cajamarca region.
China:
Imported cases with little or no possibility of ongoing mosquito transmission in Yunnan province. 19 Jul 2019. 1 case imported but country of origin not stated.
USA:
Laboratory-confirmed symptomatic Zika virus disease cases and presumptive viremic blood donors reported to ArboNET by states and mainland United States, 2019 (provisional data as of 1 Aug 2019).
WHO Zika Epidemiology Update
As of July 2019, a total of 87 countries and territories have had evidence of autochthonous mosquito-borne transmission of Zika virus (ZIKV), distributed across 4 of the 6 WHO Regions (African Region, Region of the Americas, South-East Asia Region, and Western Pacific Region). In 2018, Ethiopia was the only new country added to the list of countries with evidence of autochthonous, mosquito-borne transmission, based on a publication of a 2014 study.
Incidence of ZIKV infection in the Americas peaked in 2016 and declined substantially throughout 2017 and 2018. ZIKV transmission has been found in all countries in the Region of the Americas except mainland Chile, Uruguay, and Canada. New scientific evidence continues to accumulate and advance our understanding of global ZIKV transmission and its associated complications.
Recent studies have provided new information on the incidence, prevalence, and patterns of ZIKV transmission worldwide.
Globally, 61 countries and territories in 6 WHO regions have evidence of established competent _Aedes aegypti_ vectors but have not yet documented ZIKV transmission. Therefore, there is still the potential risk for ZIKV to spread to additional countries. It is also possible that some of these countries have or have had transmission that has not yet been detected or reported. All areas with prior reports of ZIKV transmission have the potential for re-emergence or re-introduction.
Infection with ZIKV continues to carry the risk of Guillain-Barre syndrome and adverse pregnancy outcomes, including increased risk of preterm birth, foetal death and stillbirth, and congenital malformations collectively characterized as congenital Zika syndrome (CZS).
ZIKV genetic sequence analyses have been important in elucidating patterns of global spread. The 2 major lineages of ZIKV, known as the Asian and African lineages, have been identified. The differences in the epidemic potential and pathogenicity of these viral lineages and strains are not fully understood.
Accurate and up-to-date epidemiologic data on ZIKV are limited in many areas of the world. The majority of ZIKV infections are asymptomatic, and when disease occurs, symptoms are generally mild and non-specific, and therefore may not be detected or reported.
WHO information for travellers, July 2019
Disease Research Update
Natural vertical transmission of Zika virus in larval Aedes aegypti populations, Morelos, Mexico, Journal of Emerging Infectious Diseases
Of the 151 pools of larvae researchers analyzed in Jojulta, Morelos, Mexico, 17 tested positive for Zika virus RNA; infectious Zika virus was successfully isolated from one of the larvae pools. These results demonstrate the occurrence of natural vertical transmission of Zika virus in wild Ae. Aegypti mosquitoes and suggest that this transmission mode could aid in the spread and maintenance of Zika virus in nature.
See the full ProMED post here
Information available within this Disease Outbreak Update is produced by Program for Monitoring Emerging Diseases (ProMED).
Note: Content may be edited for style and length.
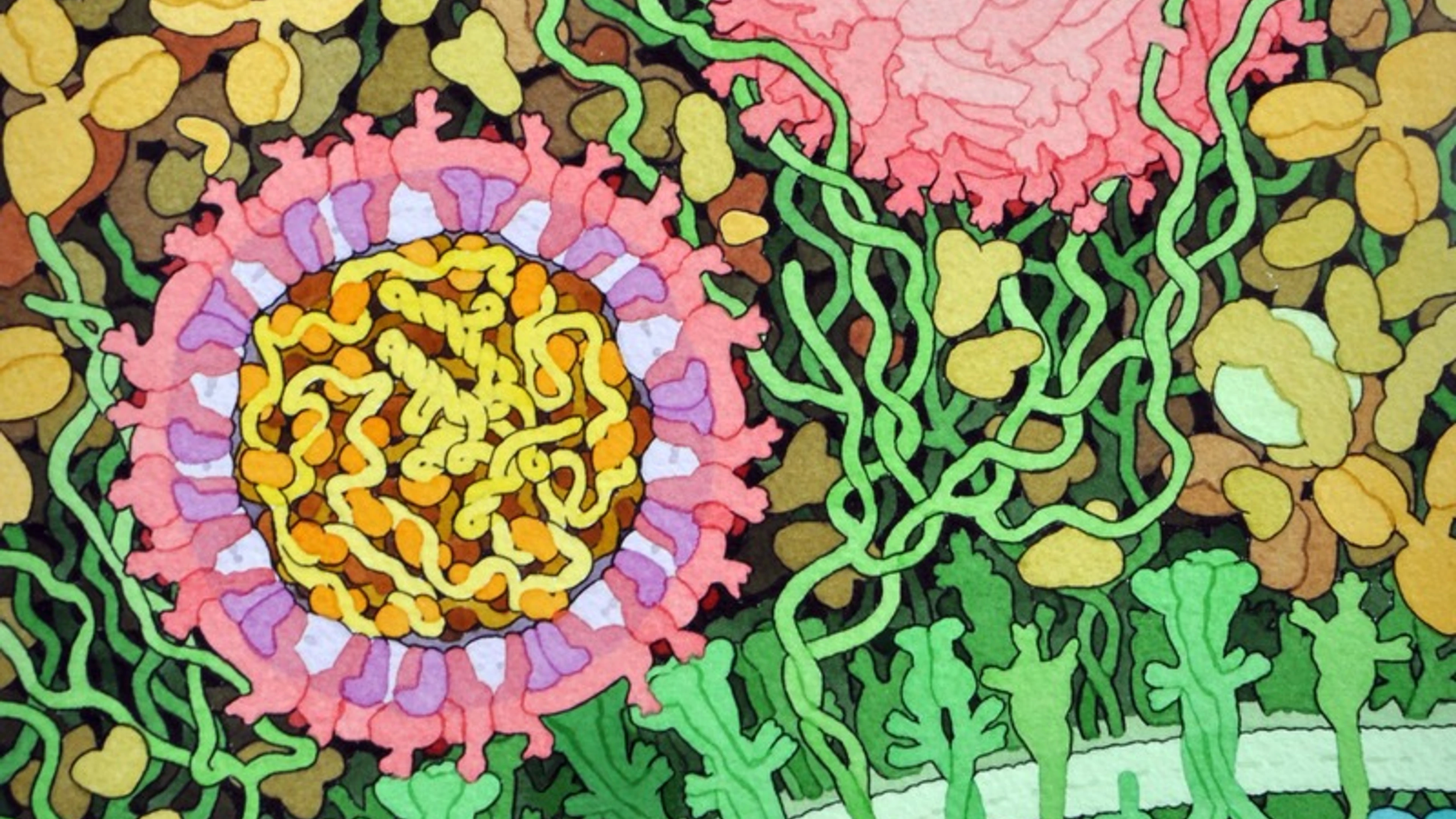
Image: Space-fill drawing of the outside of one Zika virus particle, and a cross-section through another as it interacts with a cell. The two main proteins of the viral envelope, the envelope proteins and membrane proteins, are shown in red and purple respectively. The lipid membrane of the envelope is shown in light lavender.The capsid proteins, in orange, are shown interacting with the RNA genome, in yellow, at the center of the virus. The cell-surface receptor proteins are in green, the cytoskeleton in blue, and blood plasma proteins in gold. Drawn by David Goodsell.

ProMED: Pneumonia cases of unknown cause in Wuhan, China
ProMED: MERS cases reported in Doha, Qatar